Evidence suggests that obesity accounts for up to 90% of the risk of developing type 2 diabetes.
Not everyone with type 2 diabetes is overweight or obese as defined by Body Mass Index (BMI).
E.g., indigenous people, South Asians, etc…
Central adiposity (i.e., intra-abdominal fat) is the underlying issue.
Adipose (fat) tissue stores much of the excess energy
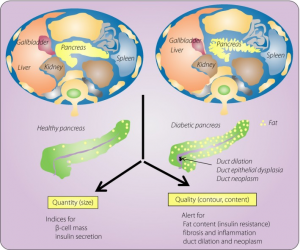
Excess fat accumulates in other organs → liver, pancreas, and muscle.
In these non–adipose tissues, excess energy leads to lipotoxicity, meaning the excess fat stored in these cells inhibits their proper functioning.
This disrupts normal glucose and insulin metabolism.
Muscle lipotoxicity inhibits glucose uptake.
This produces peripheral insulin resistance, requiring greater amounts of insulin to “push” glucose into the muscles.
This resistance is reduced with physical activity as muscle tissues consume energy (e.g., glucose) and become more responsive to insulin.
Pancreatic lipotoxicity inhibits β-cell insulin production, reducing the amount of insulin available to overcome the insulin resistance in muscles and other organs.
Significant energy restriction removes triglycerides (fat) from the pancreas in a matter of days, restoring β-cell insulin production.
This occurs before significant weight loss occurs in other organs and tissues, indicating it is not just excess body fat, but excess energy, driving insulin resistance and type 2 diabetes.
MRI scans of the pancreas in nearly 33,000 people in the UK.
Higher pancreatic fat content is associated with a 42% increase in risk of developing type 2 diabetes.
Assessing adiposity
BMI is not the best measure of excess body fat (adiposity):
– Waist circumference;
– Waist : height ratio;
– Bioimpedance analysis;
– Fat Mass Index = Fat Mass (kg) ÷ height² (m²). are much better indicators